

Overview
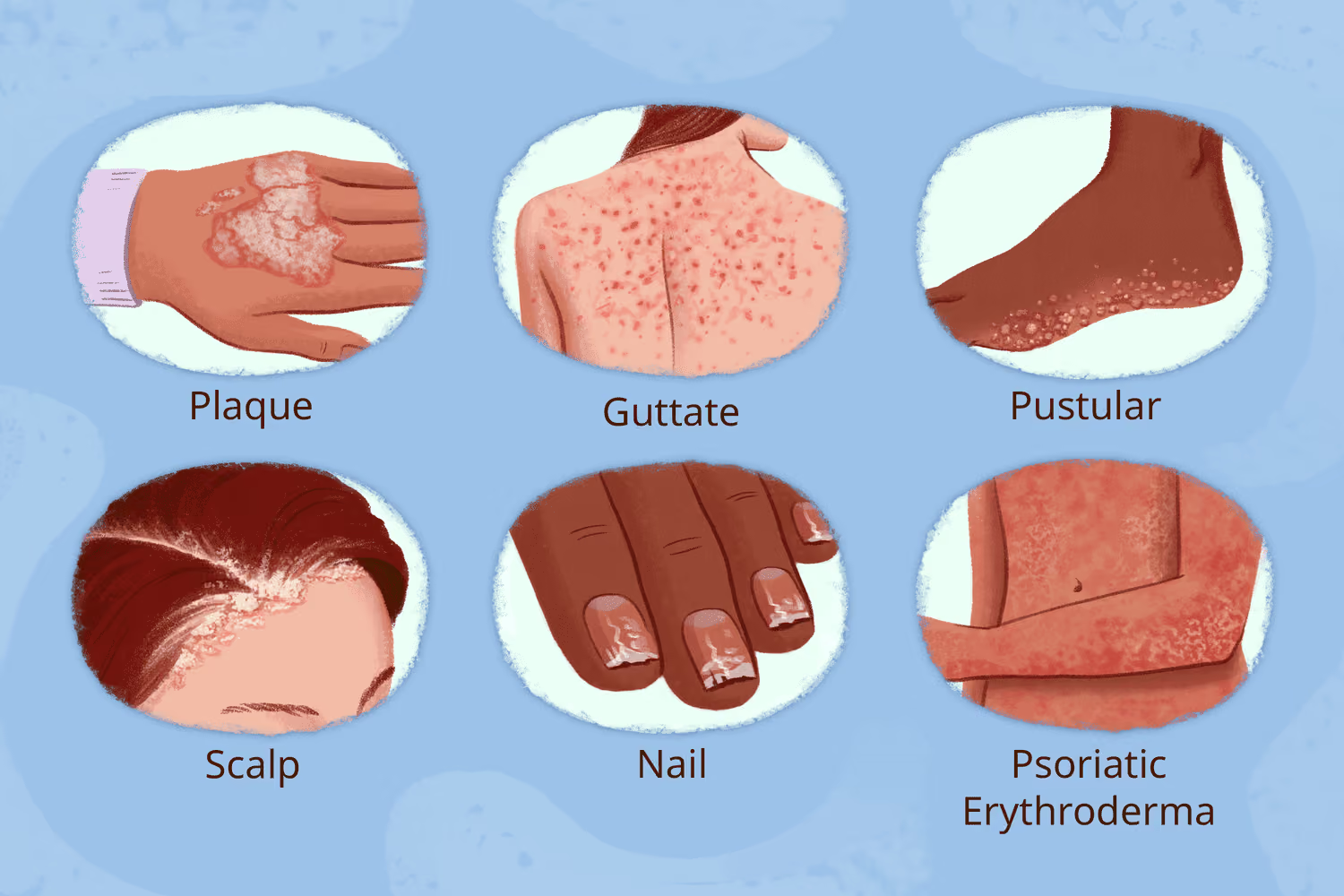
Psoriasis is a chronic, immune-mediated inflammatory disease that affects about three percent of American adults. The most familiar form, plaque psoriasis, produces well-defined patches of thick red skin covered by silvery scale, most often on the elbows, knees, scalp, and lower back. Psoriasis is not contagious, but it can be painful, itchy, and emotionally taxing, and is associated with several important systemic conditions.
Up to 30 percent of patients with skin psoriasis develop psoriatic arthritis, an inflammatory arthritis that can cause permanent joint damage if not treated. Psoriasis is also linked to cardiovascular disease, fatty liver, depression, and metabolic syndrome, which is why comprehensive care addresses more than just the skin.
At Cleaver Dermatology and Aesthetics, our board-certified dermatologists treat every form and severity of psoriasis at all nine of our offices in North Georgia and Metro Atlanta. Treatment options have expanded enormously, and most patients with moderate to severe disease can now achieve nearly clear or completely clear skin with modern biologics.
