

Overview
Melanoma is the most serious form of skin cancer because of its ability to spread to lymph nodes and distant organs. About 100,000 new invasive melanomas are diagnosed in the United States each year. The encouraging news is that when melanoma is caught early, while it is still confined to the skin, the five-year survival rate is around 99 percent. Late detection is what makes melanoma deadly, not the cancer itself.
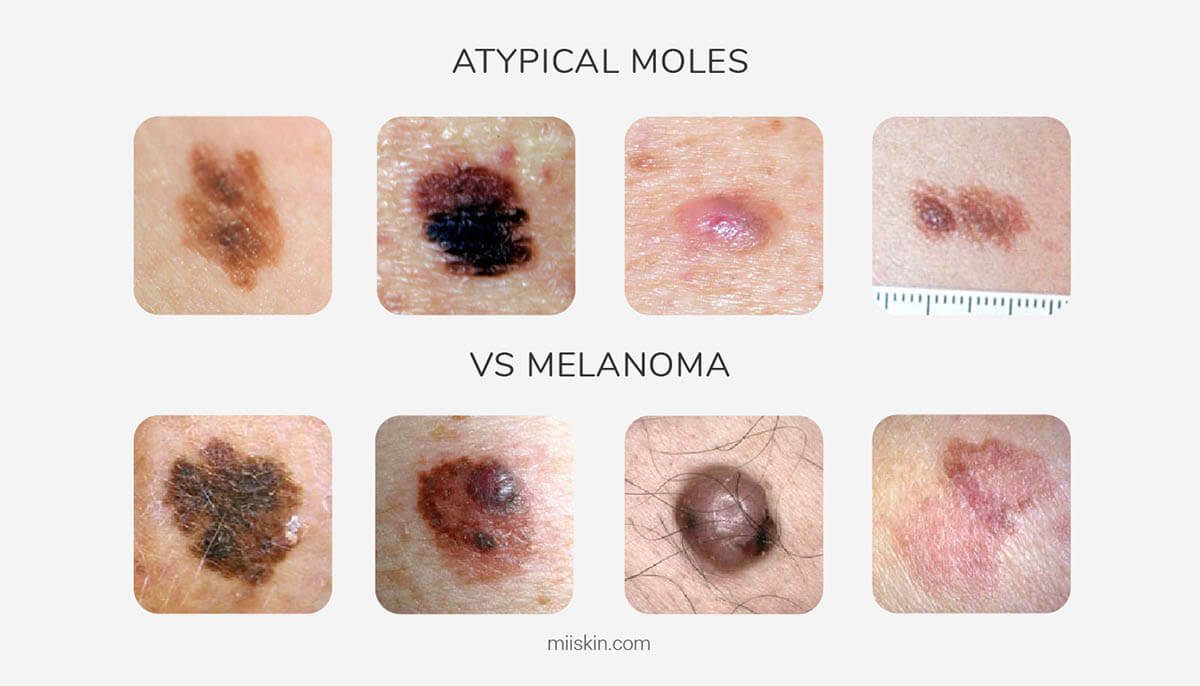
Atypical moles, also called dysplastic nevi, are unusual-looking moles that are not melanoma but do carry a higher risk of becoming melanoma over time and serve as a marker for elevated overall melanoma risk. People with multiple atypical moles, a personal or family history of melanoma, or both, benefit from regular dermatologic surveillance.
At Cleaver Dermatology and Aesthetics, our board-certified dermatologists provide full-body skin exams, dermoscopy, biopsy, and coordinated treatment for melanoma at all nine of our North Georgia and Metro Atlanta offices. We work closely with surgical oncology and medical oncology when advanced disease requires it.
